
Midwifery Course
PARTOGRAPHY or Partograph

➡️ The partogram:
CLASS OBJECTIVES:

At the end of this session the student must be able to :
Define common terms related to partograph:Pelvic outlet .
Pelvic brim(inlet) . Diagonal conjugate. Occiput.
class objectives:
molding, labour.Caput ,
Engagement,& Dilatation.
latent phase of labour.
Active phase of labour.
Partograph.
Sinciput
Vertex.
Cont: objectives:
2) Describe the partograph:
The progress of labor (cx dilataion,descent of head, uterine contraction).
The fetal conditions.
The maternal condition.
Cont:objectives:
First stage of labor (cx dilatation, latent phase, active phase)
Molding
Definitions of common terms:
PARTOGRAM:
is a graphical record card used to monitoring progress of labour, among parameters recorded are, dilatation of cervix, descent of the presenting part, foetal heart beat, contractions, blood pressure, and pulse.
These are used to monitor labour as well as the condition of mother and fetus.
Cont:definitions :
Or
PARTOGRAPH :
Is defined as a graphical record of the progress of labour and salient features of the mother and fetus.
Cont:definitions:
LABOR: Is the process by which the foetus,placenta and membranes are expelled out from the uterus.
LATENT PHASE OF LABOR: Is the early part of the first stage of labour, the cervix dilates from 0 up to 4 cm and the cx is shortens (effaced).
Cont:definitions :
ACTIVE PHASE &TRANSITION OF LABOR: Is the later part of the first stage of labour. The cx dilates from 4cm up to 10cm and the cx is very thin.
DILATATION: The opening of the cx during labour identified on vaginal examination.
Is usually measured in cm,with 0 cm being closed and 10 being fully open.
Cont:definitions:
PELVIC BRIM (inlet): The upper opening of the true pelvis. The rounded opening where the presenting part of the fetus goes into on its way to delivery.
PELVIC OUTLET: Is the lower opening of the bonny cavity. Its diamond in shaped. The most important diameter is intertuberosities which measures 11cm in a normal pelvis.
Cont:definitions of common terms:
-DIAGNAL CONJUGATE: An internal
measurements of the pelvis from the bottom of the pubic arch to sacral promontory,12 – 13cm.
OCCIPUT: The back of the babies head ,the area over the occipital bone.
SINCIPUT: The forehead of the fetus.
Cont:definitions of common terms:
VERTEX:
The area of the head between the anterior and posterior fontanels and the two parietal eminences.
Cont:definition of common terms:
ENGAGEMENT:
Is said to have occurred when the widest presenting transverse diameter has passed through the brim of the pelvic.
In cephalic presentation this is the bi-parietal diameter and in breech presentation it is the bitrochanteric diameter.
Cont:definitions of common terms:
MOULDING: The overlapping of a babies skull bone so the head can fit through the pelvis of the mother. The head is squeezed or compressed to reduce its diameter.
CAPUT: Is a swelling on the head of the fetus (caput succedaneum) due to infiltration of serum and blood into the scalp tissue.
The description of the partograph:
Observation charted on the partogram (partograph):
The parts of the partograph:
(A) MOTHER PART
(B) FERTAL PART
Which in general Include;
1.GENERAL INFORMATION OF THE MOTHER.
name,gravida,para,regestratio/hospital number, date of admission, time of admission, and time membrane ruptures.
Cont:the parts of the partograph:
2) FETAL MONITORING SECTION.
Fetal heart rate recorded to monitor fetal condition.
Liquor or amniotic fluid is observed and recorded as . “C” as clear .and “M” as meconium stained. ‘’I” as intact membrane,”R” as Ruptured membrane.
Cont:the parts of the partograph:
MOULDING OBSERVED AND RECODED AS:
“O” means no moulding
+ means small moulding
++ means moderate moulding
+++ means severe moulding
Cont:the parts of the partograph
3. LABOUR PROGRESS:
a) CX DILATATION:
plotted with an X. The latent phase, active phase, alert and action lines are also monitored.
DESCENT OF THE HEAD: Is plotted with an
“O”
Cont:the parts of the partograph
TIME : recorded as admission time zero time. The actual time of the day is recorded below the hours line.
b)PROGRESS OF LABOR AND CONTRACTION:
The contractions are recorded below the time line, along with cervical dilatation and descent of presenting part, they ball together tell the progress of labour.
Maternal monitoring (condition):
Blood pressure, pulse rate and temperature are recorded in the space provided.
Urine amount is recorded every time urine is passed. albumin(protein) and acetone are tested at least once.
medications: oxytocin,intravenous, fluids(infusion) are recorded in the space provided.
Symbols used during partograph recording:
membranes,and liquor:
I =Intact
C =clear
B =blood stained
A =abscent
M+=Light meconium
M++ = Thick meconium
Cont:symbols used during
partograph recording:
Moulding:
O = bones not touching and sutures felt easily.
+= bones just touching each other but not overlapping.
++= bones are overlapping but can be reduced.
+++= bones are touching and cannot be reduced.
Contractions:
Chart every half hour; palpate the number of contractions in 10 minutes and their duration in seconds.
(1) Less than 20 seconds:
(2) Between 20 and 40 seconds:
(3) More than 40 seconds
Oxytocin:
Record amount per volume IV fluids in drops/min. every 30 min. when used.
Drugs given:
Record any additional drugs given
Cont:symbols used during
partograph recording:
Blood pressure millimeters of mercury (mmHg)
Maternal pulse ( Mp)
Descent of presenting part (0).
Cont:symbols used during
partograph recording:
Urine, protein and acetone-nil or + or ++,+++.
Urine-amount in mls
Fluid intake-record time, type of fluid and actual amount taken in mls.
First stage of labor:
1st stage of labor is divided into the latent, and active phase:
Latent phase: Cervical dilatation:
(slow period of cervical dilatation) from 0-4cm with gradual shortening of the cervix.
Cont:first stage of labor:
dilatation of cervix is recorded with an X.
If the progress is satisfactory the plotting of
cervical dilatation will remain on to left of the alert line.
Cont:first stage of labor:
2)The active and transition phase :
(faster period of cervical dilatation) is from 4 cm to 10 cm (full cervical dilatation). dilatation is recorded with X.
If progress is satisfactory the plotting of cervical dilatation will remain on or to the left of the alert line.
Cont: 1st stage of labour:
Descent of head:
For labour to progress well, dilatation of the cervix should be accompanied by descend of the head.
Descend may not take place until cervix is 7cm dilated especially in primigravida but in multipara it may be before dilation to 7cm.
Cont: 1st stage of labour
-Descend of head is measured by abdominally in fifthly above the pelvic brim.
Assess before doing the vaginal examination.
– A head which is mobile will accommodate the full width of five fingers.
– Engaged when the bother above will accommodate s 2 fingers.
Uterine contractions
In order for labour to progress there must be good uterine contractions.
In normal labour they wholly became more frequently and last longer as labour progress.
Cont:uterine contractions:
Observation of uterine contractions:
hourly in latent phase.
half hourly in active phase.
Frequency – how often.
Duration – how long they last.
FETAL CONDITIONS:
3)Fetal condition:
Observing fetal heart rate is a safe and relative clinical way of knowing that the baby is well.
Best time is just after contractions has passed its strongest phase.
Listen to the fetal heart 1 minute when the woman is at lateral position if possible.
Cont:Fetal condition:
Fetal contractions recorded on the top of the partogram
Recorded half hourly.
Normally is between 120 – 160.
Abnormal heart rate:
>160 beats =Tachycardia
<120 beats = bradycardia this may indicate fetal distress..
Cont :abnormal heart rate:
In case abnormal fetal heart rate is heard .you have to listen at least every 15 minutes immediately after every contractions.
A heartbeat of 100 or lower indicators very severe distress and thus action must be taken at once.
4).Membrane and liquor:
The state of the liquor can assist the fetal condition.
Observations are made at each vaginal examination.
Cont:Membrane and liquor:
Presence of thick meconium at any time or abscent of liquor at the time of membrane rupture ,is the key to listen the fetal heart more frequently as these may be signs of fetal distress.
moulding of the fetal skull:
Moulding is an important indicator of telling how adequate the pelvis is to accommodate the fetal head.
Increasing moulding with the head high in the pelvis is a key sign of cephalo – pelvic dispropotion.
Moulding may difficult to assess in presence of a large caput.
caput succedaneum
/cephalohaematoma:
The meaning and its difference:
Caput succedaneum:
usually present at birth and you may feel during vaginal examination and the swelling crosses the suture line.
Cephalohaematoma appears 24 hrs after birth and the swelling does not cross the suture line.
Descending of head
*Descent assessed by abdominal palpation: Part of head (divided into 5 parts) palpable above the symphysis pubis; recorded as a circle (O) at every vaginal examination. At 0/5, the sinciput (S) is at the level of the symphysis pubis
MIDWIFERY COURSE PDF NOTES
11. Cord Prolapse and Presentation
13. Pre-eclampsia and Eclampsia
15. Risk factors occuring During Pregnancy

Zaidi ya vifo milioni 3 kila mwaka hutokana na matumizi ya pombe na madawa ya kulevya-WHO

kuharisha na kutapika ni dalili za ugonjwa gani

Dalili za mimba hutokea baada ya siku ngapi






Maumivu chini ya kitovu ni dalili za ugonjwa gani
Maumivu chini ya kitovu ni dalili za ugonjwa gani. Watu wengi huweza kupata maumivu chini ya kitovu, lakini umewahi kujiuliza...


Kaswende ni ugonjwa gani, soma hapa kufahamu
Kaswende ni ugonjwa gani, Kaswende ni maambukizi yanayosababishwa na bakteria. Mara nyingi, huenea kupitia mawasiliano ya kingono au kwa kujamiiana....


Koo kukauka ni dalili ya ugonjwa gani
Koo kukauka ni dalili ya ugonjwa gani Koo kukauka kunaweza kusababishwa na sababu kadhaa, ikiwa ni pamoja na: Upungufu wa...


Amiba ni ugonjwa gani,Fahamu kuhusu Ugonjwa wa Amebiasis
Amiba ni ugonjwa gani Wengi wamezoea kusema hivo ila Amiba(amoeba) ni vimelea vyinavyosababisha ugonjwa, na Ugonjwa huo kitaalam ndyo hujulikana...


kuwashwa nyayo za miguu husababishwa na nini? chanzo na Tiba
kuwashwa nyayo za miguu husababishwa na nini? chanzo na Tiba kuwashwa nyayo za miguu; zipo sababu nyingi ambazo huchangia shida...


Ujue Ugonjwa Wa PID (Pelvic Inflammatory Disease)
Ujue Ugonjwa Wa PID (Pelvic Inflammatory Disease) Pid ni ugonjwa gani? PID ni Maambukizi ya bacteria Kwenye Via vya Uzazi...


SHINGO YA MTOTO KULEGEA(CHANZO CHAKE)
SHINGO YA MTOTO KULEGEA(CHANZO CHAKE) Mabadiliko ya Watoto wengi huanza kwenye miezi mitatu ya Mwanzo wakati ambapo Shingo ya mtoto...


MAUMIVU MAKALI SEHEMU YA HAJA KUBWA
Baadhi ya watu wanachanganya tatizo la maumivu makali sehemu ya haja kubwa pamoja na tatizo la Bawasiri,japo mojawapo ya chanzo...


TATIZO LA MASIKIO KUPIGA KELELE,CHANZO NA TIBA YAKE(Tinnitus)
TATIZO LA MASIKIO KUPIGA KELELE,CHANZO NA TIBA YAKE(Tinnitus) tatizo la masikio kupiga kelele Tinnitus, ni Tatizo la masikio kupiga kelele,...


DALILI ZA UGONJWA WA GONO(KISONONO)
UGONJWA WA KISONONO DALILI ZA UGONJWA WA GONO(KISONONO) Ugonjwa wa gonorrhea maarufu kama GONO au Kisonono ni ugonjwa wa zinaa...


TATIZO LA UKE KUJAMBA PAMOJA NA TIBA YAKE(chanzo cha tatizo hili ni nini?)
Tatizo la Uke Kujamba TATIZO LA UKE KUJAMBA PAMOJA NA TIBA YAKE(chanzo cha tatizo hili ni nini?) Moja ya vitu...


DALILI ZA FANGASI UUMENI,KORODANI PAMOJA NA MATIBABU YAKE
FANGASI • • • • • DALILI ZA FANGASI UUMENI,KORODANI PAMOJA NA MATIBABU YAKE Mashambulizi ya Fangasi sehemu za siri...


CHANZO CHA TATIZO LA KUOTA NYAMA PUANI PAMOJA NA MATIBABU YAKE
Chanzo cha tatizo la NYAMA PUANI,Dalili zake Pamoja na Tiba yake, Soma makala hii kwa Makini ili upate Kujua kuhusu...
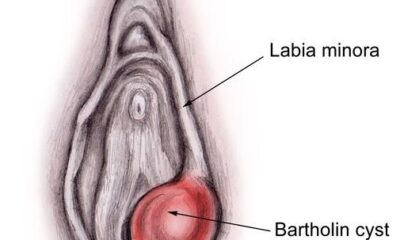

SABABU ZA KUVIMBA KWA MASHAVU YA UKE(TEZI LA BARTHOLIN)
KUVIMBA MASHAVU YA UKE • • • • • • Katika Makala hii tumechambua zaidi kuhusu sababu za kuvimba mashavu...


TATIZO LA MWANAUME KUOTA MATITI(gynecomastia)
TATIZO LA MWANAUME KUOTA MATITI(gynecomastia) Tatizo hili linatokea kwa Baadhi ya wanaume,na hata kupelekea Wanaume hao kuwa na Matiti kama...

kuharisha na kutapika ni dalili za ugonjwa gani
kuharisha na kutapika ni dalili za ugonjwa gani Unapopata tatizo la kuharisha na kutapika kwa wakati mmoja unaweza kuwaza sana,...


Dalili za infection kwenye damu,mchafuko wa damu
Dalili za infection kwenye damu Mchafuko wa damu,chanzo,dalili na Tiba Mchafuko wa damu; hiki ni kiswahili ambacho watu wamezoea kukitumia...


Ugonjwa wa ngozi sehemu za siri
Ugonjwa wa ngozi sehemu za siri Yapo magonjwa mbali mbali ya ngozi ambayo huweza kuathiri Sehemu za Siri za Mwanaume...


Dalili za acid reflux,Soma hapa Kufahamu
Dalili za acid reflux: Tatizo la Gastroesophageal reflux disease (GERD), ni tatizo ambalo huwapata Watu wengi,Tatizo hili hujulikana kwa jina...
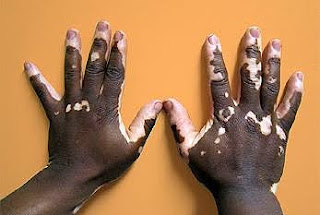

Ugonjwa wa ngozi kuwa nyeupe,VITILIGO
Ugonjwa wa ngozi kuwa nyeupe,VITILIGO Vitiligo ni ugonjwa wa ngozi kuwa nyeupe au ni ugonjwa ambao huhusisha ngozi kupoteza rangi...


Mlipuko wa ugonjwa wa macho,Macho Mekundu
Mlipuko wa ugonjwa wa macho,Macho Mekundu Baada ya Ugonjwa huu wa macho kusumbua watu wengi kwa kipindi cha Hivi Karibuni,...


Scabies ni ugonjwa gani? Soma hapa kufahamu
Scabies ni ugonjwa gani? Soma hapa kufahamu Utangulizi: Scabies huhusisha mtu kuwa na vipele na muwasho kwenye ngozi yake ambapo...


Dalili za ugonjwa wa gono kwa mwanaume
Dalili za ugonjwa wa gono kwa mwanaume Gono ni neno maarufu ambalo kirefu chake ni Gonorrhea na kiswahili chake ni...


Dalili Mpya za ukimwi kwenye ngozi
Zipi ni Dalili za ukimwi kwenye ngozi Zipi ni dalili za Ukimwi kwenye ngozi ya mtu? Fahamu hapa kupitia makala...


Madhara ya COVID-19: Athari za Ugonjwa, Asili na Matibabu
Madhara ya COVID-19: Athari za Ugonjwa, Asili na Matibabu Huu ni ugonjwa wa kuambukiza uliosababishwa na kirusi cha corona, ambao...
-

 Uzazi/Ujauzito5 days ago
Uzazi/Ujauzito5 days agoDalili za hatari baada ya kujifungua kwa upasuaji
-
Magonjwa4 days ago
Dalili za infection kwenye damu,mchafuko wa damu
-
 Uzazi/Ujauzito3 days ago
Uzazi/Ujauzito3 days agoDalili za mimba hutokea baada ya siku ngapi
-
Magonjwa7 days ago
Ugonjwa wa ngozi sehemu za siri
-
Magonjwa2 days ago
kuharisha na kutapika ni dalili za ugonjwa gani
-

 Events6 days ago
Events6 days agoChad yafanikiwa kuondoa Ugonjwa wa trypanosomiasis,WHO yatangaza
-

 News4 days ago
News4 days agoTANZIA:Yusuf Manji afariki dunia akipatiwa Matibabu Marekani
-
 Utafiti21 hours ago
Utafiti21 hours agoZaidi ya vifo milioni 3 kila mwaka hutokana na matumizi ya pombe na madawa ya kulevya-WHO